*This information was originally published as part of an abstract for the 67th ASH Annual Meeting and Exposition*
Understanding Multiple Myeloma and the Unmet Patient Need
The treatment landscape for multiple myeloma (MM) continues to expand with the introduction of bispecific antibodies (BsAbs), offering new hope for patients with relapsed or refractory MM after prior therapy. However, integrating these novel therapies into community cancer centers presents complex challenges related to clinical coordination, toxicity management, and access to multidisciplinary resources.
Despite growing familiarity with BsAbs, real-world implementation often lags behind evidence-based recommendations. Community providers cite uncertainty in adverse event (AE) management, limited patient education tools, and gaps in prognostic scoring and cytogenetic testing. These barriers underscore the need for targeted education that combines clinical data with practical, systems-based strategies to improve readiness and equitable access to advanced MM therapies.
The Medlive Approach
To address these challenges, Medlive partnered with Blood Cancer United and collaborated with experts from leading community cancer networks to design a four-phase implementation science (IS) initiative combining real-world data collection with educational interventions.
The goal was to identify barriers, align treatment practices with guidelines, and create actionable frameworks to improve bispecific antibody integration in community settings.
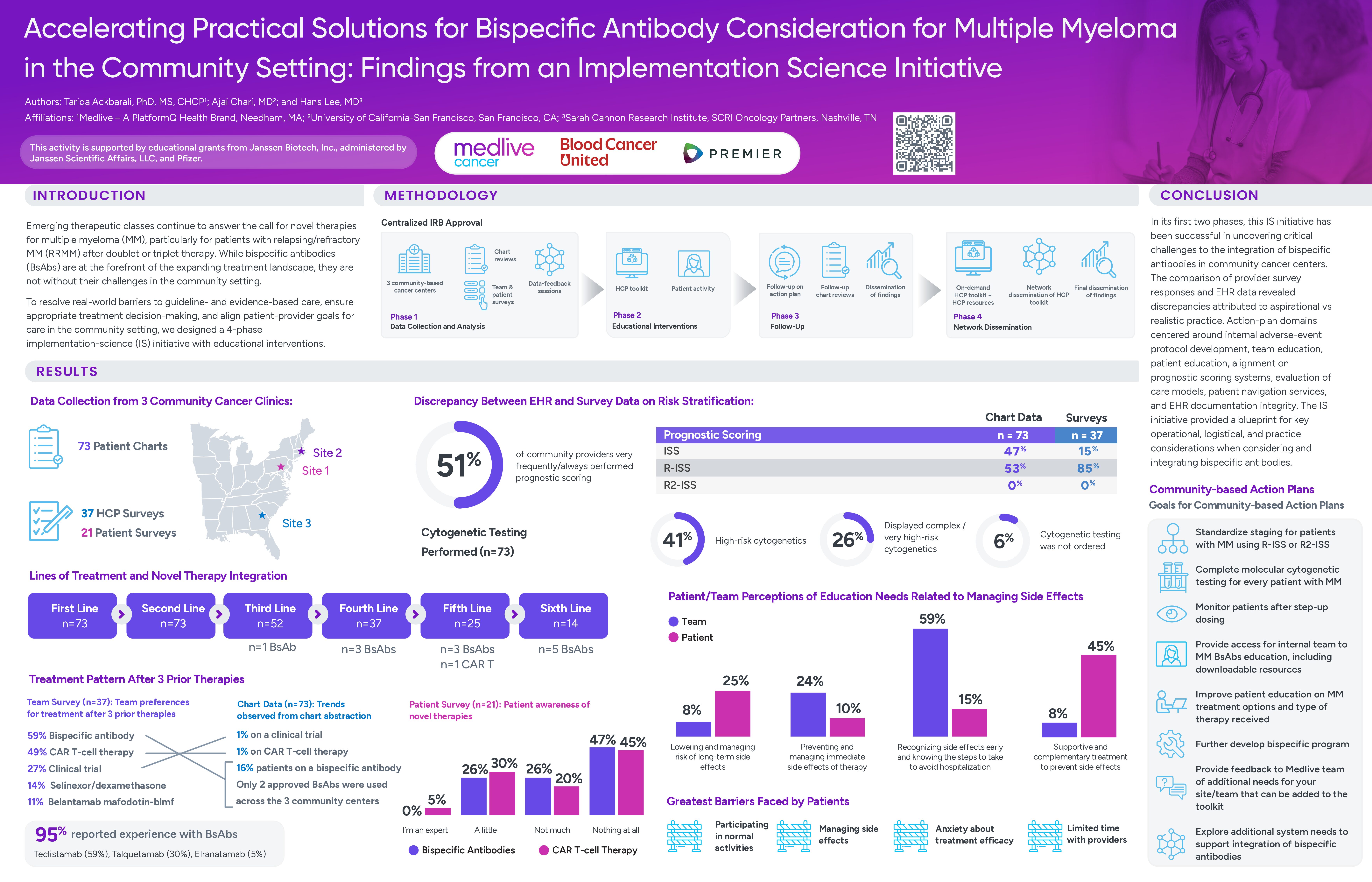
- Phase 1: Centralized IRB approval and data collection across three centers, including 73 patient charts, 37 healthcare provider (HCP) surveys, and 21 patient surveys.
- Phase 2: Data-feedback sessions and educational interventions focused on AE management, patient engagement, and prognostic scoring. Clinicians from the three centers developed site-specific action plans to standardize staging (using R-ISS or R2-ISS), enhance molecular and cytogenetic testing, and improve patient and team education regarding BsAbs.
- Phase 3: Follow-up evaluations and chart reviews to measure progress against action-plan goals.
- Phase 4: Network dissemination of findings and toolkit resources to expand best practices across additional sites.
Key Findings
The poster summarizes the findings from the first two phases, comparing provider survey responses and EHR data, and analysis of action plan domains.
- Cytogenetic testing and prognostic scoring discrepancies: 51% of community providers reported very frequent or consistent use of prognostic scoring, including specifying the scoring system used. However, we found discrepancies between surveys and chart extraction data: R-ISS was utilized in 85% of surveyed cases versus 53% in chart data, while ISS showed inverse patterns (15% surveys vs 47% charts). R2-ISS was not documented in either dataset, suggesting potential gaps in adoption of updated staging systems or inconsistencies between reported and actual clinical practice. Looking at cytogenetic testing, 41% of charts showed high cytogenetics, 26% showed complex or very high cytogenetics, and 6% of the cases had no cytogenetic testing ordered.
- Treatment integration: For patients with three or more prior lines of therapy, survey respondents would use bispecific antibodies (59%) or CAR T-cell therapy (49%), while chart abstraction showed only 16% of patients actually received bispecific antibodies, 1% received CAR T-cell therapy, and 1% were enrolled in clinical trials.
- Bispecific antibody experience: 95% reported experience with BsAbs, 59% with teclistamab, 30% talquetamab, and 5% elranatamab. However, only BsAbs and CAR T were used across the three sites.
- Patient education needs: Nearly half of surveyed patients reported no awareness of CAR T or BsAbs. Most patients prioritized learning to recognize side effects early (59%) and improving access to supportive treatments (45%), while providers highlighted the need for clearer toxicity management pathways and standardized AE monitoring.
- Action plan domains: centered around internal adverse-event protocol development, team education, patient education, alignment on prognostic scoring systems, evaluation of care models, patient navigation services, and EHR documentation integrity.
Conclusion – Advancing Readiness for Bispecific Antibody Use in Community Settings
This initiative revealed critical gaps between perceived and actual readiness to integrate bispecific antibodies for MM treatment in community practices. Comparison of survey and chart data highlighted aspirational versus realistic practice patterns, emphasizing the importance of implementation support alongside education.
Site-specific action plans—focused on AE management, cytogenetic testing, team education, and patient navigation—created a blueprint for optimizing operational readiness and improving access to BsAbs. Continued collaboration among community teams, educators, and advocacy partners such as Blood Cancer United will be key to sustaining progress and ensuring high-quality, equitable care for patients with multiple myeloma.
To learn more about partnering with Medlive, reach out via our Contact Us page.
This activity was supported by educational grants from Janssen Biotech, Inc., administered by Janssen Scientific Affairs, LLC, and Pfizer.


